
Page 80 - GPD-4-2
P. 80
Gene & Protein in Disease Alport syndrome: Genetics, variability, and management
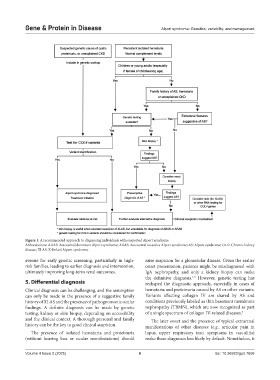
Figure 1. A recommended approach to diagnosing individuals with suspected Alport syndrome
Abbreviations: ADAS: Autosomal dominant Alport syndrome; ARAS: Autosomal recessive Alport syndrome; AS: Alport syndrome; CKD: Chronic kidney
disease; XLAS: X-linked Alport syndrome.
avenue for early genetic screening, particularly in high- raise suspicion for a glomerular disease. Given the earlier
risk families, leading to earlier diagnosis and intervention, onset presentation, patients might be misdiagnosed with
ultimately improving long-term renal outcomes. IgA nephropathy, and only a kidney biopsy can make
the definitive diagnosis. However, genetic testing has
1,3
5. Differential diagnosis reshaped the diagnostic approach, especially in cases of
Clinical diagnosis can be challenging, and the assumption hematuria and proteinuria caused by AS or other variants.
can only be made in the presence of a suggestive family Variants affecting collagen IV are shared by AS and
history of XLAS and the presence of pathognomonic ocular conditions previously labeled as thin basement membrane
findings. A definite diagnosis can be made by genetic nephropathy (TBMN), which are now recognized as part
testing, kidney or skin biopsy, depending on accessibility of a single spectrum of collagen IV-related diseases. 3
and the clinical context. A thorough personal and family The later onset and the presence of typical extrarenal
history can be the key to good clinical suspicion. manifestations of other diseases (e.g., articular pain in
The presence of isolated hematuria and proteinuria lupus, upper respiratory tract symptoms in vasculitis)
(without hearing loss or ocular manifestations) should make these diagnoses less likely by default. Nonetheless, it
Volume 4 Issue 2 (2025) 6 doi: 10.36922/gpd.7656