
Page 105 - ITPS-8-2
P. 105
INNOSC Theranostics and
Pharmacological Sciences Fungal markers in intracranial fungal infections
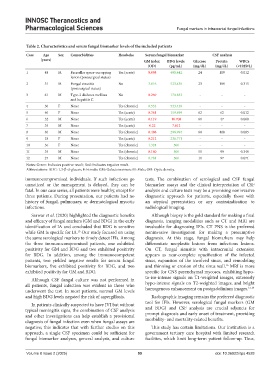
Table 2. Characteristics and serum fungal biomarker levels of the included patients
Case Age Sex Comorbidities Headache Serum fungal biomarker CSF analysis
(years) GM index BDG levels Glucose Protein WBCs
(OD) (pg/mL) (mg/dL) (mg/dL) (×10E9/L)
1 48 M Parasellar space-occupying Yes (acute) 0.098 408.442 24 109 0.012
lesion (postsurgical status)
2 51 M Fungal sinusitis No 3.016 523.438 23 189 0.315
(postsurgical status)
3 61 M Type-2 diabetes mellitus No 0.269 170.833 - - -
and hepatitis C
4 30 F None Yes (chronic) 0.533 523.438 - - -
5 40 F None Yes (acute) 0.361 159.899 62 62 0.012
6 32 M None Yes (acute) 0.119 10.708 61 47 0.008
7 35 M None Yes (acute) 0.22 7.812 - - -
8 40 M None Yes (chronic) 0.488 298.994 60 408 0.085
9 18 F None Yes (acute) 0.212 236.771 - - -
10 36 F None Yes (chronic) 1.324 500 - - -
11 35 M None Yes (chronic) 0.160 500 51 99 0.340
12 27 M None Yes (chronic) 0.781 500 11 97 0.071
Notes: Green: Indicates positive result; Red: Indicates negative result.
Abbreviations: BDG: 1,3-β-d-glucan; F: Female; GM: Galactomannan; M: Male; OD: Optic density.
immunocompromised individuals. If such infections go tests. The combination of serological and CSF fungal
unnoticed or the management is delayed, they can be biomarker assays and the clinical interpretation of CSF
fatal. In our case series, all patients were healthy, except for analysis and culture tests may be a promising noninvasive
three patients. During presentation, our patients had no diagnostic approach for patients, especially those with
history of fungal, pulmonary, or dermatological mycotic an atypical presentation or any contraindication to
infections. radiological imaging.
Sarwar et al. (2020) highlighted the diagnostic benefits Although biopsy is the gold standard for making a final
and efficacy of fungal markers (GM and BDG) in the early diagnosis, imaging modalities such as CT and MRI are
identification of IA and concluded that BDG is sensitive invaluable for diagnosing IFIs. CT PNS is the preferred
while GM is specific for IA. Our study focused on using noninvasive investigation for making a presumptive
15
the same serological markers to timely detect IFIs. Among diagnosis. At this stage, fungal biomarkers may help
the three immunocompromised patients, one exhibited differentiate neoplastic lesions from infectious lesions.
positivity for GM and BDG and two exhibited positivity On CT, fungal sinusitis with intracranial extension
for BDG. In addition, among the immunocompetent appears as near-complete opacification of the infected
patients, two yielded negative results for serum fungal sinus, expansion of the involved sinus, and remodeling
biomarkers, five exhibited positivity for BDG, and two and thinning or erosion of the sinus wall. MRI is more
16
exhibited positivity for GM and BDG. specific for CNS parenchymal mycoses, exhibiting hypo-
Although CSF fungal culture was not performed in to-iso-intense signals on T1-weighted images, extremely
all patients, fungal infection was evident in those who hypo-intense signals on T2-weighted images, and bright
17,18
underwent the test. In most patients, normal GM levels homogenous enhancement on postgadolinium images.
and high BDG levels negated the risk of aspergillosis. Radiographic imaging remains the preferred diagnostic
In patients clinically suspected to have IVI but without tool for IFIs. However, serological fungal markers (GM
typical meningitis signs, the combination of CSF analysis and BDG) and CSF analysis are crucial adjuncts for
and other investigations can help establish a provisional prompt diagnosis and early onset of treatment, providing
diagnosis of fungal infection even when fungal assays are morbidity- and mortality-related benefits.
negative; this indicates that with further studies on this This study has certain limitations. Our institution is a
approach, a single CSF specimen could be sufficient for government tertiary care hospital with limited research
fungal biomarker analyses, general analysis, and culture facilities, which limit long-term patient follow-up. Thus,
Volume 8 Issue 2 (2025) 99 doi: 10.36922/itps.4528