
Page 9 - AN-2-2
P. 9
Advanced Neurology Venous stenting, intracranial hypertension
and infections are less likely although the average cost for When IIH is refractory to management, several
stenting is higher . criteria must be met before performing CVSS. The major
[22]
criteria include a pressure gradient of 8 mmHg or more
A B across the stenosis, intracranial pressure of 22 mmHg or
more, no contraindication to dual antiplatelet therapy
(clopidogrel and aspirin), and the presence of one or
more of the following symptoms: severely disabling
headache, focal neurological deficit, papilledema, or
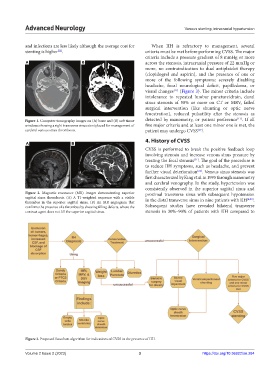
visual changes [17] (Figure 3). The minor criteria include
intolerance to repeated lumbar puncture/drain, dural
sinus stenosis of 50% or more on CT or MRV, failed
surgical intervention (like shunting or optic nerve
fenestration), reduced pulsatility after the stenosis as
Figure 1. Computer tomography images on (A) bone and (B) soft tissue detected by manometry, or patient preference [17] . If all
windows showing a right transverse sinus stent placed for management of five major criteria and at least one minor one is met, the
cerebral venous sinus thrombosis. patient may undergo CVSS [17] .
4. History of CVSS
A B
CVSS is performed to break the positive feedback loop
involving stenosis and increase venous sinus pressure by
treating the focal stenosis . The goal of the procedure is
[21]
to reduce IIH symptoms, such as headache, and prevent
further visual deterioration . Venous sinus stenosis was
[21]
first characterized by King et al. in 1995 through manometry
and cerebral venography. In the study, hypertension was
consistently observed in the superior sagittal sinus and
Figure 2. Magnetic resonance (MR) images demonstrating superior proximal transverse sinus with subsequent hypotension
sagittal sinus thrombosis. (A) A T1-weighted sequence with a visible in the distal transverse sinus in nine patients with IIH [4,23] .
thrombus in the superior sagittal sinus. (B) An MR angiogram that
confirms the presence of a thrombus by showing filling defects, where the Subsequent studies have revealed bilateral transverse
contrast agent does not fill the superior sagittal sinus. stenosis in 30%–90% of patients with IIH compared to
Figure 3. Proposed flowchart algorithm for indications of CVSS in the presence of IIH.
Volume 2 Issue 2 (2023) 3 https://doi.org/10.36922/an.284