
Page 70 - OR-1-1
P. 70
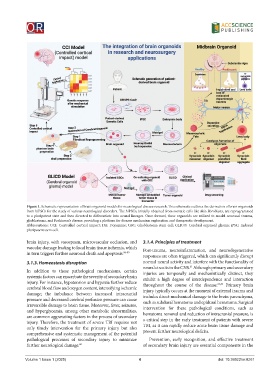
Figure 1. Schematic representation of brain organoid models for neurological disease research. This schematic outlines the derivation of brain organoids
from hiPSCs for the study of various neurological disorders. The hiPSCs, initially obtained from somatic cells like skin fibroblasts, are reprogrammed
to a pluripotent state and then directed to differentiate into neural lineages. Once formed, these organoids are utilized to model neuronal trauma,
glioblastoma, and Parkinson’s disease, providing a platform for disease mechanism exploration and therapeutic development.
Abbreviations: CCI: Controlled cortical impact; DA: Dopamine; GSC: Glioblastoma stem cell; GLICO: Cerebral organoid glioma; iPSC: Induced
pluripotent stem cell.
brain injury, with vasospasm, microvascular occlusion, and 3.1.4. Principles of treatment
vascular damage leading to local brain tissue ischemia, which Post-trauma, neuroinflammation, and neurodegenerative
in turn triggers further neuronal death and apoptosis. 56-59 responses are often triggered, which can significantly disrupt
3.1.3. Homeostasis disruption normal neural activity and interfere with the functionality of
neural circuits in the CNS. Although primary and secondary
61
In addition to these pathological mechanisms, certain injuries are temporally and mechanistically distinct, they
systemic factors can exacerbate the severity of secondary brain exhibit a high degree of interdependence and interaction
injury. For instance, hypotension and hypoxia further reduce throughout the course of the disease. 62,63 Primary brain
cerebral blood flow and oxygen content, intensifying ischemic injury typically occurs at the moment of external trauma and
damage; the imbalance between increased intracranial includes direct mechanical damage to the brain parenchyma,
pressure and decreased cerebral perfusion pressure can cause such as subdural hematoma and epidural hematoma. Surgical
irreversible damage to brain tissue. Moreover, fever, seizures, intervention for these pathological conditions, such as
and hyperglycemia, among other metabolic abnormalities, hematoma removal and reduction of intracranial pressure, is
are common aggravating factors in the process of secondary
injury. Therefore, the treatment of severe TBI requires not a critical step in the early treatment of patients with severe
only timely intervention for the primary injury but also TBI, as it can rapidly reduce acute brain tissue damage and
comprehensive and systematic management of the potential prevent further neurological deficits.
pathological processes of secondary injury to minimize Prevention, early recognition, and effective treatment
further neurological damage. 60 of secondary brain injury are essential components in the
Volume 1 Issue 1 (2025) 4 doi: 10.36922/or.8261