
Page 27 - AIH-1-1
P. 27
Artificial Intelligence in Health NLP in EHR
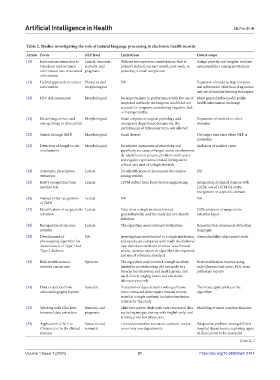
Table 2. Studies investigating the role of natural language processing in electronic health records
Article Focus NLP level Limitations Future scope
[15] Information extraction to Lexical, semantic, Without retrospective consideration, that is, Assign priority and weights; evaluate
transform unstructured syntactic and patient’s status from past month, past week, or interoperability among institutions
information into structured pragmatic yesterday; a small sample size
information
[19] Hybrid approach to extract Phonetics and NA Expansion of model to larger corpora
information morphological and information other than drug names
and use of machine learning techniques
[20] HIV risk assessment Morphological No improvement in performance with the use of More generalizable model public
empirical methods; the unigram model did not health information exchange
account for unigram, considering negation, lack
of interoperability
[21] Identifying correct and Morphological Small corpora of surgical pathology and Expansion of method to other
mis-spellings in clinical text emergency department documents, the domains
performance of infrequent term sets affected
[22] Search through EMR Morphological Small dataset Use larger data sizes when NLP is
preferable
[23] Detection of fungal ocular Morphological No relative assessment of sensitivity and Inclusion of positive cases
involvement specificity, no cases of fungal ocular involvement,
de-identification process, problems with query
and regular expression, limited for inpatient
critical care unit of a single institute
[24] Automatic prescription Lexical De-identification of documents the relation NA
extraction among entities
[25] Entity recognition from Lexical LSTM suffers from fussy feature engineering Integration of clinical domain with
medical text LSTM, use of LSTM for entity
recognition in a specific domain
[26] Named entity recognition Lexical NA NA
in EMR
[27] Identification of surgical site Lexical Data from a single institute limited Differentiation of surgical site
infection generalizability, and the study did not classify infection types
infection
[28] Recognition of syncope Lexical The algorithm needs external verification Reproduction of research with other
patients languages
[29] Development of NA Investigations were limited to a single institution, Generalizability of proposed work
phenotyping algorithm for and results are compared with multi-institutional
identification of Type 1 and case definition methods, institute-wise limited
Type 2 diabetes access, iterative nature of algorithm development,
and use of reference standard
[30] Risk stratification in Syntactic The algorithm only involved a single institute, Risk stratification beyond using
prostate cancer care limited to prostatectomy, did not apply to a only Gleason total score, PSA, from
broader health system and health group, and pathology reports
used clinical staging forms and electronic
laboratory records
[31] Data extraction from Semantic Extraction of data elements with qualitative The broad applicability of the
echocardiography reports value, extracted data require manual review, algorithm
tested at a single institute, inclusion/exclusion
criteria for the study
[32] Working with CliniText, Semantic and CliniText system deals with only structured data, Modeling of more complex domains
temporal data extraction pragmatic excluding images, testing with English only, and
is limited to a few physicians
[33] Application of NLP to Syntactic and Limited annotation resources, syntactic corpus Adaptation problem among differed
Chinese text in the clinical semantic cover only two departments hospital departments, exploring types
domain of clinical text to be annotated
(Cont’d...)
Volume 1 Issue 1 (2024) 21 https://doi.org/10.36922/aih.2147