
Page 10 - GTM-2-1
P. 10
Global Translational Medicine Mineralocorticoid receptor in CMD
2.2. Role of DC MR in hypertension identified as a specific target of MR in cardiovascular
DCs are activated and increased in the secondary cells [50-52] . The specific knockout of DC NGAL can
lymphoid tissue of hypertensive mice treated with Ang effectively inhibit MR-dependent T cell activation and
[50]
II infusion or DOCA salt . The specific ablation of DCs inflammatory response .
[43]
(CD11c-expressing cells) prevents the development of 2.3. T cell MR and CMDs
hypertension as a result of Ang II infusion [44,45] . MR is
also expressed and functional in DCs . MR activation 2.3.1. Role of T cell MR in hypertension
[46]
in DCs promotes the differentiation of T cells into The previous animal models and clinical studies have
pro-inflammatory Th1 and Th17 phenotypes and decreases demonstrated that T cells play a key role in mediating renal
the proportion of regulatory T cells (Tregs) (Figure 2). This and vascular inflammation and hypertension [53,54] . The role
imbalance between T helper cells and Tregs contributes of T cell MR in hypertension has been investigated. In Ang
to the pathogenesis of hypertension and its associated II-infused mice, the deletion of MR in T cells strikingly
complications [47,48] . Further experiments have shown that decreases both systolic and diastolic blood pressures and
aldosterone pretreatment activates DCs, promotes the attenuates renal and vascular damages . In contrast,
[27]
expression of DC maturation markers CD80 and CD86, the overexpression of MR in T cells increases blood
and induces DCs to secrete cytokines such as IL-6 and pressure in response to Ang II infusion . Mechanically,
[27]
IL-23, thereby activating CD4 and CD8 T cells . These MR in T cells, particularly CD8 T cells, interacts with
[46]
+
+
+
activated T cells then migrate to the kidney and vasculature, transcription factors nuclear factor of activated T cells
producing interferon gamma (IFNγ) and IL-17A and 1 (NFAT1) and AP-1 to regulate IFNγ production,
exacerbating hypertension (Figure 2). Spironolactone, and ultimately influences blood pressure (Figure 2).
[49]
[27]
an MR antagonist, effectively inhibits DC activation, T cell Consistently, eplerenone, which is also an MR antagonist,
immunity, and the development of hypertension [30,46] . attenuates AngII-induced hypertension and decreases
Araos et al. have provided information concerning IFNγ expression in CD8 T cells . Other studies have
+
[27]
the downstream mechanisms of DC MR activation in a shown that T cell MR is involved in the regulation of
nephrectomy-aldosterone-salt model of hypertension . renal fibrosis and blood pressure in DOCA/salt-induced
[50]
MR stimulation in DCs favors neutrophil gelatinase- hypertension model by regulating the expression of C-X-C
associated lipocalin (NGAL) and IL-23 expression, which chemokine receptor type 4 (CXCR4) [55,56] . As reported,
are involved in the development of fibrosis and Th17 mineralocorticoid excess stimulates the accumulation of T
response, respectively (Figure 2). NGAL has been cells in the kidney, which is significantly blunted by CXCR4
[50]
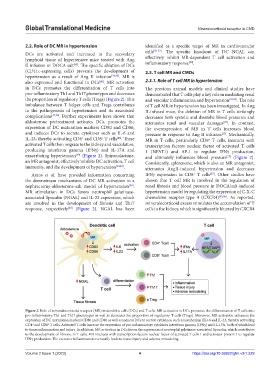
Figure 2. Role of mineralocorticoid receptor (MR) in dendritic cells (DCs) and T cells. MR activation in DCs promotes the differentiation of T cells into
pro-inflammatory Th1 and Th17 phenotypes as well as decreases the proportion of regulatory T cells (Tregs). Moreover, MR activation enhances the
expression of DC maturation markers CD80 and CD86 as well as induces DCs to secrete cytokines, such as interleukin (IL)-6 and IL-23, thereby activating
CD4 and CD8 T cells. Activated T cells increase the expression of pro-inflammatory cytokines Interferon gamma (IFNγ) and IL-17A, both of which lead
+
+
to tissue inflammation and injury. In addition, MR activation in DCs favors the expression of neutrophil gelatinase-associated lipocalin, which contributes
to the development of fibrosis. In T cells, MR interacts with transcription factors nuclear factor of activated T cells 1 and activator protein 1 to regulate
IFNγ production. The excessive inflammation eventually leads to tissue injury and adverse remodeling.
Volume 2 Issue 1 (2023) 4 https://doi.org/10.36922/gtm.v2i1.229