
Page 111 - IJPS-10-3
P. 111
International Journal of
Population Studies Gender differences in mental health outcomes
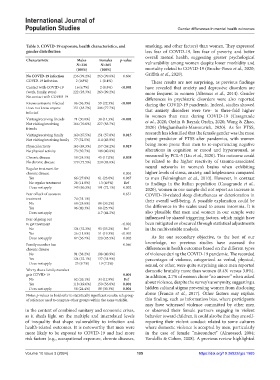
Table 3. COVID‑19 exposure, health characteristics, and smoking, and other factors) than women. They expressed
gender distribution less fear of COVID-19, less fear of poverty, and better
overall mental health, suggesting greater psychological
Characteristic Males Females p‑value
N=238 N=265 vulnerability among women despite lower morbidity and
(100%) (100%) mortality related to COVID-19 (Broche-Perez et al., 2020;
No COVID‑19 infection 236 (99.2%) 263 (99.6%) 0.606 Griffith et al., 2020).
COVID-19 infection 2 (0.8%) 1 (0.4%) These results are not surprising, as previous findings
Contact with COVID-19 16 (6.7%) 2 (0.8%) <0.001 have revealed that anxiety and depressive disorders are
(work, family, store) 222 (93.3%) 263 (99.2%) more frequent in women (Altemus et al., 2014). Gender
No contact with COVID-19 differences in psychiatric disorders were also reported
Knows someone infected 86 (36.3%) 59 (22.3%) <0.001 during the COVID-19 pandemic. Indeed, studies showed
Does not know anyone 151 (63.7%) 206 (77.7%) that anxiety disorders were two- to three-fold higher
infected in women than men during COVID-19 (Casagrande
Visiting/receiving friends 71 (30.0%) 38 (14.3%) <0.001 et al., 2020; Ozdin & Bayrak Ozdin, 2020; Wang & Zhao,
Not visiting/receiving 166 (70.0%) 227 (85.7%)
friends 2020) (Moghanibashi-Mansourieh, 2020). As for PTSS,
Visiting/receiving family 160 (67.5%) 151 (57.0%) 0.015 research has identified that the female gender was the most
Not visiting/receiving family 77 (32.5%) 114 (43.0%) potent predictor of PTSS after pandemics, with women
Physical activity 165 (69.3%) 157 (59.2%) 0.019 being more prone than men to re-experiencing negative
No physical activity 73 (30.7%) 108 (40.8%) alterations in cognition or mood and hyperarousal, as
Chronic disease 58 (24.5%) 45 (17.0%) 0.038 measured by PCL-5 (Liu et al., 2020). This outcome could
No chronic disease 179 (75.5%) 220 (83.0%) be related to the higher reactivity of trauma-associated
Regular treatment for neural networks in women’s brains when exhibiting
chronic disease 0.004 higher levels of stress, anxiety, and helplessness compared
Yes 66 (27.8%) 61 (23.0%) 0.067 to men (Felmingham et al., 2010). However, in contrast
No regular treatment 28 (11.8%) 13 (4.9%) Ref to findings in the Italian population (Casagrande et al.,
Does not apply 143 (60.3%) 191 (72.1%) 0.002 2020), women in our sample did not report an increase in
Fear of lack of access to 0.651 COVID-19-related sleep disturbances or deterioration in
treatment 74 (31.1%) their overall well-being. A possible explanation could be
No 68 (28.6%) 80 (30.2%)
Yes 96 (40.3%) 68 (25.7%) the difference in the scales used to assess insomnia. It is
Does not apply 117 (44.2%) also plausible that men and women in our sample were
Fear of going out influenced by shared triggering factors, which might have
to get treatment <0.001 been mitigated or obscured through statistical adjustments
No 124 (52.3%) 93 (35.2%) Ref in the multivariable analysis.
Yes 26 (11.0%) 51 (19.3%) <0.001
Does not apply 87 (36.7%) 120 (45.5%) 0.002 As for our secondary objective, to the best of our
Family member has 0.566 knowledge, no previous studies have assessed the
chronic disease differences in health outcomes based on the different types
No 91 (38.2%) 108 (40.9%) of violence during the COVID-19 pandemic. The recorded
Yes 124 (52.1%) 137 (51.9%) percentages of violence, categorized as verbal, physical,
Does not apply 23 (9.7%) 19 (7.2%) sexual, or other, were quite surprising since men reported
Worry that a family member domestic brutality more than women (8.4% versus 3.8%).
gets COVID-19 0.001 In addition, 2.7% of women chose “no answer” when asked
No 62 (26.1%) 34 (12.9%) Ref
Yes 118 (49.6%) 150 (56.8%) 0.001 about violence, despite the survey’s anonymity, suggesting a
Does not apply 58 (24.4%) 80 (30.3%) 0.001 hidden cultural stigma preventing women from disclosing
Notes: p-values in bold refer to statistically significant results; ref: group abuse (Francis et al., 2017). Other factors may explain
of reference used to compare other groups within the same variable. this finding, such as information bias, where participants
may have witnessed violence committed by other men
in the context of combined sanitary and economic crises, or observed their female partners engaging in violent
as it sheds light on the multiple and interrelated levels behavior toward children. It could also be that they are self-
of inequality that shape vulnerability to infection and reporting their violent conduct related to some cultures
health-related outcomes. It is noteworthy that men were where domestic violence is accepted by men, particularly
more likely to be exposed to COVID-19 and had more in the case of female “misconduct” (Almosaed, 2004;
risk factors (e.g., occupational exposure, chronic diseases, Vandello & Cohen, 2008). A previous review highlighted
Volume 10 Issue 3 (2024) 105 https://doi.org/10.36922/ijps.1985