
Page 68 - AN-2-4
P. 68
Advanced Neurology A novel marker for healthy intracranial arteries
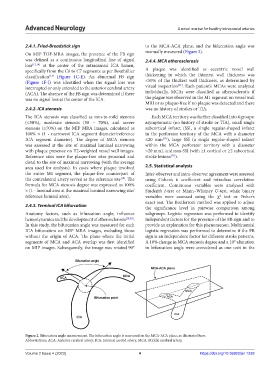
2.4.1. Fried-Breadstick sign to the MCA-ACA plane, and the bifurcation angle was
On MIP TOF-MRA images, the presence of the FB sign manually measured (Figure 2).
was defined as a continuous longitudinal line of signal 2.4.4. MCA atherosclerosis
loss [12,16] at the center of the intracranial ICA lumen,
specifically from the C6 to C7 segments as per Bouthillier A plaque was identified as eccentric vessel wall
classification (Figure 1C-E). An abnormal FB sign thickening in which the thinnest wall thickness was
[17]
(Figure 1F-I) was identified when the signal loss was <50% of the thickest wall thickness, as determined by
[21]
interrupted or only extended to the anterior cerebral artery visual inspection . Each patient’s MCAs were analyzed
(ACA). The absence of the FB sign was determined if there individually. MCAs were classified as atherosclerotic if
was no signal loss at the center of the ICA. the plague was observed in the M1 segment on vessel wall
MRI or as plaque-free if no plaque was detected and there
2.4.2. ICA stenosis was no history of strokes or TIA.
The ICA stenosis was classified as non-to-mild stenosis Each MCA territory was further classified into 4 groups:
(≤50%), moderate stenosis (50 – 70%), and severe asymptomatic (no history of stroke or TIA), small single
stenosis (≥70%) on the MIP MRA images, calculated as subcortical infarct (SSI, a single regular-shaped infarct
100% × (1 - narrowest ICA segment diameter/reference in the perforator territory of the MCA with a diameter
ICA segment diameter). The degree of MCA stenosis ≤20 mm ), large SSI (a single regular-shaped infarct
[22]
was assessed at the site of maximal luminal narrowing within the MCA perforator territory with a diameter
with plaque presence on T2-weighted vessel wall images. >20 mm), and non-SSI (with ≥1 cortical or ≥2 subcortical
Reference sites were the plaque-free sites proximal and stroke lesions ).
[23]
distal to the site of maximal narrowing (with the average
area used for analysis). In cases where plaque involved 2.5. Statistical analysis
the entire M1 segment, the plaque-free counterpart of Inter-observer and intra-observer agreement were assessed
the contralateral artery served as the reference site . The using Cohen’s κ coefficient and intraclass correlation
[18]
formula for MCA stenosis degree was expressed as 100% coefficient. Continuous variables were analyzed with
× (1 - luminal area at the maximal luminal narrowing site/ Student’s t-test or Mann–Whitney U-test, while binary
reference luminal area). variables were assessed using the χ test or Fisher’s
2
exact test. The Bonferroni method was applied to adjust
2.4.3. Terminal ICA bifurcation the significance level in pairwise comparison among
Anatomy factors, such as bifurcation angle, influence subgroups. Logistic regression was performed to identify
hemodynamics and the development of atherosclerosis [19,20] . independent factors for the presence of the FB sign and to
In this study, the bifurcation angle was measured for each provide an explanation for this phenomenon. Multinomial
ICA bifurcation on MIP MRA images, excluding those logistic regression was performed to determine if the FB
without the origin of ACA. The plane where the initial sign is an independent factor for different stroke patterns.
segments of MCA and ACA overlap was first identified A 10% change in MCA stenosis degree and a 10° alteration
on MIP images. Subsequently, the image was rotated 90° in bifurcation angle were considered as one unit in the
Figure 2. Bifurcation angle measurement. The bifurcation angle is measured on the MCA-ACA plane, as illustrated here.
Abbreviations: ACA: Anterior cerebral artery; ICA: Internal carotid artery; MCA: Middle cerebral artery.
Volume 2 Issue 4 (2023) 4 https://doi.org/10.36922/an.1238