
Page 120 - EJMO-9-1
P. 120
Eurasian Journal of Medicine and
Oncology
HEART and SYNTAX scores
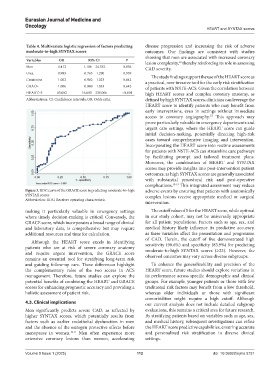
Table 4. Multivariate logistic regression of factors predicting disease progression and increasing the risk of adverse
moderate‑to‑high SYNTAX scores outcomes. Our findings are consistent with studies
showing that men are associated with increased coronary
Variables OR 95% CI P lesion complexity, thereby reinforcing its role in assessing
12
Men 4.412 1.186 – 24.332 0.036 CAD severity.
Urea 0.993 0.765 – 1.290 0.959
The study findings support the use of the HEART score as
Creatinine 1.002 0.982 – 1.023 0.842 a practical, non-invasive tool for the early risk stratification
GRACE 1.006 0.980 – 1.033 0.642 of patients with NSTE-ACS. Given the correlation between
HEART≥5 63.002 16.603 – 239.066 <0.001 high HEART scores and complex coronary anatomy, as
Abbreviations: CI: Confidence intervals; OR: Odds ratio. defined by high SYNTAX scores, clinicians can leverage the
HEART score to identify patients who may benefit from
early interventions, even in settings without immediate
access to coronary angiography.¹⁵ This approach may
prove particularly valuable in emergency departments and
urgent care settings, where the HEART score can guide
initial decision-making, potentially directing high-risk
cases toward comprehensive imaging and intervention.
Incorporating the HEART score into routine assessments
for patients with NSTE-ACS can streamline care pathways
by facilitating prompt and tailored treatment plans.
Moreover, the combination of HEART and SYNTAX
scores may provide insights into post-intervention patient
outcomes, as high SYNTAX scores are generally associated
with substantial procedural risk and post-operative
complications. 13-15 This integrated assessment may reduce
Figure 3. ROC curve of the GRACE score in predicting moderate-to-high adverse events by ensuring that patients with anatomically
SYNTAX scores complex lesions receive appropriate medical or surgical
Abbreviation: ROC: Receiver operating characteristic.
intervention.
making it particularly valuable in emergency settings The cutoff value of 5 for the HEART score, while optimal
where timely decision-making is critical. Conversely, the in our study cohort, may not be universally appropriate
GRACE score, which incorporates a broad range of clinical for all patient populations. Factors such as age, sex, and
and laboratory data, is comprehensive but may require medical history likely influence its predictive accuracy,
additional resources and time for calculation. as these variables affect the presentation and progression
of CAD. Herein, the cutoff of five demonstrated high
Although the HEART score excels in identifying
patients who are at risk of severe coronary anatomy sensitivity (90.6%) and specificity (83.9%) for predicting
and require urgent intervention, the GRACE score moderate-to-high SYNTAX scores (≥23). However, the
remains an essential tool for stratifying long-term risk observed outcomes may vary across diverse subgroups.
and guiding follow-up care. These differences highlight To enhance the generalizability and precision of the
the complementary roles of the two scores in ACS HEART score, future studies should explore variations in
management. Therefore, future studies can explore the its performance across specific demographic and clinical
potential benefits of combining the HEART and GRACE groups. For example, younger patients or those with few
scores for enhancing prognostic accuracy and providing a traditional risk factors may benefit from a low threshold,
holistic assessment of patient risk. whereas older individuals or those with significant
comorbidities might require a high cutoff. Although
4.3. Clinical implications our current analysis does not include detailed subgroup
Men significantly predicts severe CAD, as reflected by evaluations, this remains a critical area for future research.
higher SYNTAX scores, which potentially results from By stratifying patients based on variables such as age, sex,
factors such as earlier endothelial dysfunction in men and medical history, subsequent investigations can refine
and the absence of the estrogen protective effects before the HEART score predictive capabilities, ensuring accurate
menopause in women. 10,11 Men often experience more and personalized risk stratification in diverse clinical
extensive coronary lesions than women, accelerating settings.
Volume 9 Issue 1 (2025) 112 doi: 10.36922/ejmo.5731