
Page 47 - JCTR-9-5
P. 47
Iyngkaran et al. | Journal of Clinical and Translational Research 2023; 9(5): 347-356 349
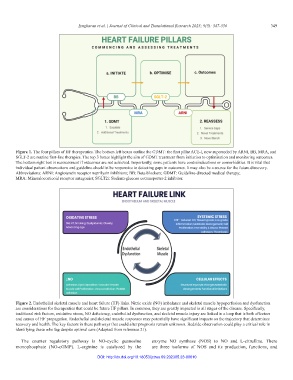
Figure 1. The four pillars of HF therapeutics. The bottom left boxes outline the GDMT: the first pillar ACE-I, now superseded by ARNI, BB, MRA, and
SGLT-2 are routine first-line therapies. The top 3 boxes highlight the aim of GDMT treatment from initiation to optimisation and monitoring outcomes.
The bottom right box is reassessment if outcomes are not achieved. Importantly, some patients have contraindications or comorbidities. It is vital that
individual patient observations and guideline checklist be responsive to detecting gaps in outcomes. It may also be a source for the future discovery.
Abbreviations: ARNI: Angiotensin receptor neprilysin inhibitors; BB: Beta-blockers; GDMT: Guideline-directed medical therapy;
MRA: Mineralocorticoid receptor antagonist; SGLT2i: Sodium-glucose cotransporter-2 inhibitor.
Figure 2. Endothelial skeletal muscle and heart failure (HF) links. Nitric oxide (NO) imbalance and skeletal muscle hypoperfusion and dysfunction
are considerations for therapeutics that could be future HF pillars. In common, they are greatly impacted in all stages of the disease. Specifically,
traditional risk factors, oxidative stress, NO deficiency, endothelial dysfunction, and skeletal muscle injury are linked in a loop that is both effectors
and causes of HF propagation. Endothelial and skeletal muscle responses may potentially have significant impacts on the trajectory that determines
recovery and health. The key factors in these pathways that could alter prognosis remain unknown. Bedside observation could play a critical role in
identifying those who lag despite optimal care (Adapted from reference 21).
The counter regulatory pathway is NO-cyclic guanosine enzyme NO synthase (NOS) to NO and L-citrulline. There
monophosphate (NO-cGMP). L-arginine is catalyzed by the are three isoforms of NOS and its production, functions, and
DOI: http://dx.doi.org/10.18053/jctres.09.202305.23-00010