
Page 8 - JCTR-9-6
P. 8
372 Sempere-Rubio et al. | Journal of Clinical and Translational Research 2023; 9(6): 369-380
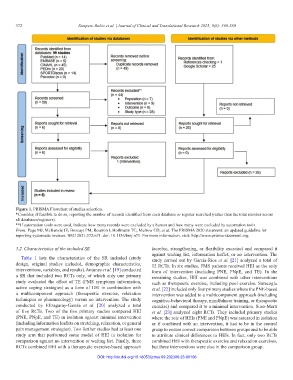
Figure 1. PRISMA Flowchart of studies selection.
*Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across
all databases/registers).
**If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.
From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for
reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org.
3.2. Characteristics of the included SR (aerobic, strengthening, or flexibility exercise) and compared it
against waiting list, information leaflet, or no intervention. The
Table 1 lists the characteristics of the SR included (study study carried out by García-Ríos et al. [21] analyzed a total of
design, original studies included, demographic characteristics, 12 RCTs. In six studies, FMS patients received HEI as the only
interventions, variables, and results). Antunes et al. [19] conducted form of intervention (including PNE, PNpE, and TE). In the
a SR that included two RCTs only, of which only one primary remaining studies, HEI was combined with other interventions
study evaluated the effect of TE (FMS symptoms information, such as therapeutic exercise, including pool exercise. Saracoglu
active coping strategies) as a form of HEI in combination with et al. [22] included only four primary studies where the PNE-based
a multicomponent approach (therapeutic exercise, relaxation intervention was added to a multicomponent approach (including
techniques or pharmacology) versus no intervention. The study cognitive-behavioral therapy, mindfulness training, or therapeutic
conducted by Elizagaray-García et al. [20] analyzed a total exercise) and compared it to a minimal intervention. Suso-Martí
of five RCTs. Two of the five primary studies compared HEI et al. [23] analyzed eight RCTs. They included primary studies
(PNE, PNpE, and TE) in isolation against minimal intervention where the role of HEIs (PNE and PNpE) was assessed in isolation
(including information leaflets on stretching, relaxation, or general or if combined with an intervention, it had to be in the control
pain management strategies). Two further studies had at least one group to ensure correct comparison between groups and to be able
study arm that performed some model of HEI in isolation for to attribute clinical differences to HEIs. In fact, only two RCTs
comparison against no intervention or waiting list. Finally, three combined HEI with therapeutic exercise and relaxation exercises,
RCTs combined HEI with a therapeutic exercise-based approach but these interventions were also in the comparison group.
DOI: http://dx.doi.org/10.18053/jctres.09.202306.23-00108