
Page 44 - AN-2-2
P. 44
Advanced Neurology Seizures and CKD
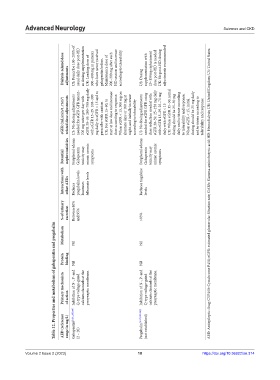
Dialysis‑related dose adjustments US: Prescribe 100–200% of usual daily dose post-HD as dosing supplementation UK: Loading dose of 300–400 mg in patients who have never received gabapentin before. Maintenance dose of 200–300 mg after each HD session and increase according to tolerability. US: Dosing supplementation with 25–150mg replacement dose post-HD is needed UK: No post-HD dosing adjustments recommended
eGFR (mL/min/1.73m 2 ) related dose adjustments US: No dosing adjustments needed for eGFR GFR tment– 700 mg twice per day with eGFR 30–59. 200–700 mg daily with eGFR 15–29. 100–300 mg daily in eGFR < 15 and to prescribe with caution UK: For eGFR 15–60, to start at low dose and increase dose according to response. When eGFR < 15, 300 mg on alternate days or 100 mg at night, and initially increase according to tolerability
Potential nephrotoxicities Peripheral edema Gabapentin toxicity may mimic uremic symptoms Peripheral edema Gabapentin toxicity may mimic uremic symptoms
Interactions with other AEDs Reduces pregabalin levels Increases felbamate levels Reduces tiagabine levels AED: Antiepileptic drug; CYP450: Cytochrome P450; eGFR: estimated glomerular filtration rate; GABA: Gamma-aminobutyric acid; HD: Hemodialysis; UK: United Kingdom; US: United States.
% of urinary excretion Between 80% and 95% >95%
Table 12. Properties and metabolism of gabapentin and pregabalin
Metabolism Nil Nil
Protein binding Nil Nil
Primary mechanism of action Inhibition of N-, P- and Q-type voltage-gated calcium channels at the presynaptic membrane. Inhibition of N-, P- and Q-type voltage-gated calcium channels at the presynaptic membrane.
AED (reference range in mg/L) Gabapentin [9,131,135,166] (2 – 20) Pregabalin [9,130,131,135] (not established)
18
https://doi.org/10.36922/an.314
V 18 https://doi.org/10.36922/an.314
Volume 2 Issue 2 (2023) olume 2 Issue 2 (2023)