
Page 39 - AN-2-2
P. 39
Advanced Neurology Seizures and CKD
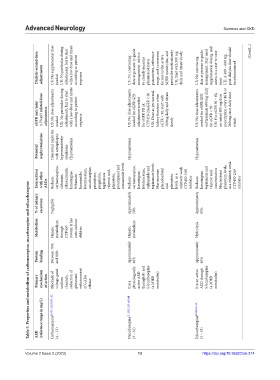
Dialysis‑related dose adjustments US: No supplemental dose needed UK: No particular dosing adjustments, but to start with a low dose and titrate according to patient response US: No convincing data at present to guide management. Advice to closely monitor pharmacokinetic parameters, reference range, and conversion factors to the active MHD metabolite, and prescribe meticulously UK: Start with 300 mg daily and titrate sl
eGFR (mL/min/ 1.73 m 2 ) related dose adjustments US: No dose adjustments needed UK: No particular dosing adjustments, but to start with a low dose and titrate according to patient response US: No dose adjustments needed for eGFR GFR adjustments needed for eGFR FR ak CYP450-2AeGFR < 30 UK: Dose as per normal kidney function when eGFR < 30, start with 300mg daily and titrate slowly US: No dose adjustments needed for eGF
Potential nephrotoxicities Interstitial nephritis with antiepileptic hypersensitivity syndrome Hyponatremia Hyponatremia Hyponatremia
Interactions with other AEDs Reduces carbamazepine, clobazam, ethosuximide, lamotrigine, felbamate, lacosamide, levetiracetam, oxcarbazepine, primidone, pregabalin, topiramate valproic acid, phenytoin, perampanel and zonisamide levels Reduces carbamazepine, lamotrigine, levetiracetam, rufinamide and topiramate levels May increase phenobarbital and phenytoin levels, as a relatively weak CYP450-2A9
Table 5. Properties and metabolism of carbamazepine, oxcarbazepine and eslicarbazepine
% of urinary excretion Negligible Approximately 50% Approximately 92%
Metabolism Hepatic metabolism through CYP450 system; it has auto-inducer abilities Hepatic metabolism Hydrolysis
Protein binding Between 70% and 80% Approximately 40% Approximately 40%
Primary mechanism of action Blockade of voltage-gated sodium channels, reduction of glutamate, enhancement of GABA release It is a physiologically active AED through R- and S-licarbazepine (a MHD metabolite) It is an active AED through S-licarbazepine (a MHD metabolite)
(reference range in mg/L) Carbamazepine [9,130-132,135,139,142] Oxcarbazepine [9,130,131,139,143,144] Eslicarbazepine [9,130,135,145]
AED (4 – 12) (3 – 35) (3 – 35)
13
https://doi.org/10.36922/an.314
Volume 2 Issue 2 (2023) olume 2 Issue 2 (2023)
V 13 https://doi.org/10.36922/an.314