
Page 42 - AN-2-2
P. 42
Advanced Neurology Seizures and CKD
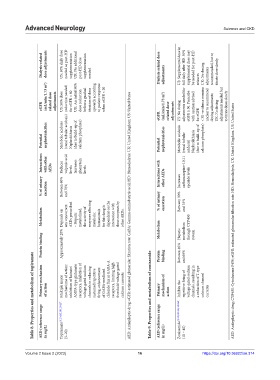
Dialysis‑related dose adjustments US: 50% daily dose needed as post-HD supplementation UK: No additional post-HD dose supplementation needed Dialysis‑related dose adjustments US: Supplemental dose in full daily after HD. 50% supplemental dose may be needed for post-HD seizures UK: No dosing adjustments recommended, but to titrate dose slowly
(mL/min/1.73 m 2 ) reduction needed UK: An initial 50% dose reduction before a gradual titration of dose upwards according to patient response when eGFR < 20
eGFR related dose adjustments US: 50% dose for eGFR < 60 eGFR (mL/min/1.73 m 2 ) related dose adjustments US: No dosing adjustments needed for eGFR ≥ 30. Prescribe with caution advised for eGFR < 30 –evidence remains unclear to recommend dosing adjustments UK: No dosing adjustments needed but to titrate doses slowly
Potential nephrotoxicities Metabolic acidosis (renal tubular acidosis) Nephrolithiasis (due to build-up of calcium phosphate) Potential nephrotoxicities Metabolic acidosis (renal tubular acidosis) Nephrolithiasis (due to build-up of calcium phosphate)
Interactions with other AEDs Reduces valproic acid levels Increases phenytoin levels Interactions with carbamazepine-10,11
% of urinary excretion Between 60% and 70% % of urinary other AEDs Increases Between 30% epoxide levels
Metabolism Depends on any concurrent AEDs prescribed – Hepatic metabolized, the activity of enzymes affecting metabolic homeostasis for this drug is dependent on the interaction with these enzymes by other AEDs. AED: Antiepileptic drug; eGFR: estimated glomerular filtration rate; GABA: Gamma-aminobutyric acid; HD: Hemodialysis; UK: United Kingdom; US: United States Metabolism excretion and 35% metabolism through CYP450
Protein binding Approximately 20% Protein binding Hepatic Between 40% and 60% system
Table 8. Properties and metabolism of topiramate
Primary mechanism of action Multiple major mechanisms of action: inhibition of kainate/ AMPA-type glutamate receptors, inhibition of voltage-gated sodium channels in reducing sustained repetitive firing, enhancement of GABA-mediated chloride flux at GABA-A receptors, limiting high threshold voltage-gated calcium currents Table 9. Properties and metabolism of zonisamide Primary mechanism of action Inhibits the repetit
AED (reference range in mg/L) Topiramate [9,130,135,139,156,157] (5–20) AED (reference range in mg/L) Zonisamide [9,130,131,135,158,159] (10 – 40)
16
https://doi.org/10.36922/an.314
Volume 2 Issue 2 (2023) olume 2 Issue 2 (2023)
V 16 https://doi.org/10.36922/an.314