
Page 41 - AN-2-2
P. 41
Advanced Neurology Seizures and CKD
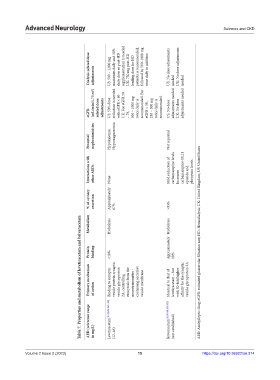
Dialysis‑related dose adjustments US: 500 – 1,000 mg maximum daily and 50% daily dose as post-HD supplementation is needed UK: 750 mg post-HD loading dose for HD patients is recommended, followed by 500–1000 mg once daily in addition US: No dose adjustments needed UK: No dose adjustments needed
(mL/min/1.73 m 2 ) related dose US: 50% dose reduction is needed with eGFR < 60 UK: For eGFR 50 500 – 1000 mg recommended. For recommended. adjustments needed adjustments needed
eGFR adjustments – 79, twice daily is eGFR < 50, 250 – 500 mg twice daily is US: No dose UK: No dose
Potential nephrotoxicities Hypokalemia Hypomagnesemia Not reported
Interactions with other AEDs None Mild reduction of carbamazepine levels Increases carbamazepine-10,11 epoxide and phenytoin levels
% of urinary excretion Approximately 67% >95%
Metabolism Hydrolysis Hydrolysis
Table 7. Properties and metabolism of levetiracetam and brivaracetam
Protein binding <10% Approximately 18% AED: Antiepileptic drug; eGFR: estimated glomerular filtration rate; HD: Hemodialysis; UK: United Kingdom; US: United States
Primary mechanism of action Binding to synaptic vesicle protein synaptic vesicle glycoprotein 2A, controlling exocytosis from the neurotransmitter - containing secretory vesicle membrane Identical to that of levetiracetam – but with 30-fold higher affinity for the synaptic vesicle glycoprotein 2A
AED (reference range in mg/L) Levetiracetam [9,130,131,147-151] (12–46) Brivaracetam [9,129,130,152-155] (not established)
15
https://doi.org/10.36922/an.314
Volume 2 Issue 2 (2023) olume 2 Issue 2 (2023)
V 15 https://doi.org/10.36922/an.314