
Page 117 - GHES-3-2
P. 117
Global Health Economics and
Sustainability
Hospitalizations due to obesity and deaths from diabetes
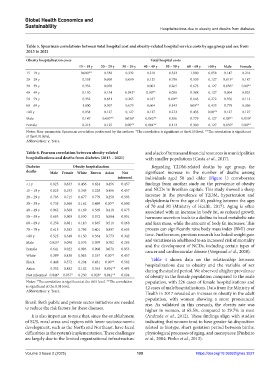
Table 5. Spearman correlations between total hospital cost and obesity‑related hospital service costs by age group and sex from
2013 to 2021
Obesity hospitalization costs Total hospital costs
15 – 19 y 20 – 29 y 30 – 39 y 40 – 49 y 50 – 59 y 60 – 69 y >80 y Male Female
15 – 19 y 0.000** 0.538 0.332 0.218 0.332 1.000 0.058 0.147 0.218
20 – 29 y 0.538 0.000 0.099 0.125 0.798 0.539 0.127 0.013* 0.187
30 – 39 y 0.332 0.050 0.002 0.265 0.673 0.127 0.036* 0.00**
40 – 49 y 0.130 0.154 0.042* 0.00** 0.058 0.388 0.127 0.004 0.025
50 – 59 y 0.332 0.831 0.265 0.187 0.00** 0.143 0.272 0.356 0.112
60 – 69 y 1.000 0.507 0.673 0.604 0.143 0.00** 0.433 0.779 0.360
>80 y 0.058 0.127 0.127 0.127 0.272 0.433 0.00** 0.127 0.127
Male 0.147 0.007** 0.036* 0.002** 0.356 0.779 0.127 0.00** 0.050*
Female 0.218 0.125 0.00** 0.004** 0.112 0.360 0.127 0.050* 0.00**
Notes: Non-parametric Spearman correlation performed by the authors. *The correlation is significant at the 0.05 level. **The correlation is significant
at the 0.01 level.
Abbreviation: y: Years.
Table 6. Pearson correlation between obesity‑related and a lack of human and financial resources in municipalities
hospitalizations and deaths from diabetes (2013 – 2021) with smaller populations (Costa et al., 2017).
Diabetes Obesity hospitalization Regarding T2DM-related deaths by age group, the
deaths Male Female White Brown Asian Not significant increase in the number of deaths among
informed individuals aged 50 and older (Figure 1) corroborates
<1 y 0.825 0.633 0.456 0.624 0.456 0.457 findings from another study on the prevalence of obesity
15 – 19 y 0.825 0.193 0.345 0.228 0.456 0.457 and NCDs in Brazilian capitals. This study showed a sharp
20 – 29 y 0.703 0.715 0.677 0.779 0.259 0.593 increase in the prevalence of T2DM, hypertension and
30 – 39 y 0.735 0.568 0.162 0.499 0.00** 0.800 dyslipidemia from the age of 40, peaking between the ages
of 70 and 80 (Ministry of Health, 2017). Aging is often
40 – 49 y 0.962 0.560 0.169 0.569 0.419 0.875 associated with an increase in body fat, as reduced growth
50 – 59 y 0.693 0.509 0.530 0.572 0.584 0.951 hormone secretion leads to a decline in basal metabolic rate
60 – 69 y 0.258 0.881 0.110 0.835 0.510 0.168 and lean mass, while the amount of body fat increases. This
70 – 79 y 0.615 0.383 0.796 0.401 0.897 0.603 process can significantly raise body mass index (BMI) over
>80 y 0.525 0.340 0.150 0.364 0.773 0.342 time. Furthermore, previous research has linked weight gain
Male 0.025* 0.098 0.576 0.079 0.782 0.283 and variations in adulthood to an increased risk of mortality
and the development of NCDs, including certain types of
Female 0.641 0.922 0.993 0.908 0.071 0.953 cancer and cardiovascular disease (Vergnaud et al., 2008).
White 0.389 0.438 0.083 0.337 0.00** 0.457
Table 4 shows data on the relationship between
Black 0.448 0.572 0.204 0.451 0.00** 0.582 hospitalizations due to obesity and the variable of sex
Asian 0.352 0.482 0.102 0.363 0.001** 0.493 during the studied period. We observed a higher prevalence
Not informed 0.046* 0.037* 0.230 0.028* 0.041** 0.104 of obesity in the female population compared to the male
Notes: *The correlation is significant at the 0.05 level. **The correlation population, with 226 cases of female hospitalizations and
is significant at the 0.01 level. 42 cases of male hospitalizations. Data from the Ministry of
Abbreviation: y: Years.
Health in 2017 revealed an increase in obesity in the adult
population, with women showing a more pronounced
Brazil. Both public and private sector initiatives are needed rise. As validated in this research, the obesity rate was
to reduce the risk factors for these diseases. higher in women, at 65.5%, compared to 29.7% in men
It is also important to note that, since the establishment (Andrade et al., 2012). These findings align with studies
of SUS, rural areas and regions with lower socioeconomic indicating that women tend to have greater fat disposition
development, such as the North and Northeast, have faced related to biotype, short gestation period between births,
difficulties in the system’s implementation. These challenges physiological processes of aging, and menopause (Pinheiro
are largely due to the limited organizational infrastructure et al., 2004; Pinho et al., 2013).
Volume 3 Issue 2 (2025) 109 https://doi.org/10.36922/ghes.3027