
Page 50 - AIH-1-4
P. 50
Artificial Intelligence in Health A fuzzy system for heartbeat classification
by medical professionals for more than 70 years to identify medical professionals are responsible for this task. This
heart conditions, such as arrhythmias. The heart’s rhythm extra workload compounds the fatigue that medical staff
1
and bioelectrical activity are expressed in an ECG. Adults already experience, raising the risk of medical errors.
typically have a resting heart rate between 60 and 100 Furthermore, a large percentage of the received ECG
beats/min. A lower resting heart rate typically indicates recordings are often false alarms, as remote monitoring
improved cardiovascular fitness and more effective cardiac devices are highly sensitive to ECG abnormalities and may
function. An athlete who has received proper training, for not effectively filter out significant cardiovascular events.
instance, may typically have a resting heart rate of about As a result, helping doctors interpret ECGs has become
40 beats/min. In contrast, heart disease can alter the shape increasingly important.
and characteristics of the heartbeats seen in an ECG, Every year, millions of ECG recordings are taken
resulting in significant deviations from the normal pattern. globally, with most being automatically processed and
Cardiac arrhythmias are common in CVDs, and their deciphered by computers. This places pressure on the
accurate classification is crucial, as successful treatment ECG interpretation techniques to be patient- and device-
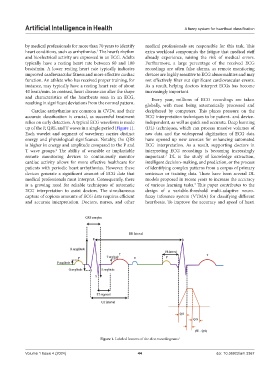
relies on early detection. A typical ECG waveform is made independent, as well as quick and accurate. Deep learning
up of the P, QRS, and T waves in a single period (Figure 1). (DL) techniques, which can process massive volumes of
Each wavelet and segment of waveform carries distinct raw data and the widespread digitization of ECG data
energy and physiological significance. Notably, the QRS have opened up new avenues for enhancing automated
is higher in energy and amplitude compared to the P and ECG interpretation. As a result, supporting doctors in
2
T wave groups. The ability of wearable or implantable interpreting ECG recordings is becoming increasingly
remote monitoring devices to continuously monitor important. DL is the study of knowledge extraction,
3
cardiac activity allows for more effective healthcare for intelligent decision-making, and prediction, or the process
patients with periodic heart arrhythmias. However, these of identifying complex patterns from a corpus of primary
devices generate a significant amount of ECG data that sentences or training data. There have been several DL
medical professionals must interpret. Consequently, there models proposed in recent years to increase the accuracy
is a growing need for reliable techniques of automatic of various learning tasks. This paper contributes to the
4
ECG interpretation to assist doctors. The simultaneous design of a variable-threshold multi-adaptive neuro-
capture of copious amounts of ECG data requires efficient fuzzy inference system (VTMA) for classifying different
and accurate interpretation. Doctors, nurses, and other heartbeats. To improve the accuracy and speed of heart
Figure 1. Labeled features of the electrocardiograms 1
Volume 1 Issue 4 (2024) 44 doi: 10.36922/aih.3367